Bridging the Recruitment Gap for Socioeconomically Disadvantaged Groups in Clinical Trials


Image credit: putilov_denis | stock.adobe.com

It should not be surprising that clinical trials remain largely inaccessible to the vast majority of patients in the United States. In fact, according to a meta analytic study, structural and clinical barriers to trial participation make trial participation unachievable, on average, for three out of four cancer patients.1
In recent years, there have been growing calls for clinical trials to account for the diverse lived experiences of different populations and make participation in these trials more accessible.2 This endeavor to recruit underrepresented populations has expanded to include socioeconomically disadvantaged groups, such as people who are lower income and less educated.
Existing research suggests that clinical trials do not adequately represent socioeconomically disadvantaged people. One study revealed that those who participate in clinical trials tend to be 65 years of age or older and have at least a college level of education, suggesting that current recruitment strategies may be skewed towards targeting people who are higher on the socioeconomic ladder.3
Indeed, more educated and higher income individuals may be perceived as more likely to comprehend the study requirements and adhere to the study protocol, highlighting a preference among study stakeholders—referring clinicians and study recruiters—to target this population at the expense of their less educated and lower income counterparts.4
What this tendency highlights is a potential bias among gatekeepers—key stakeholders, including referring clinicians and leaders who have input into the recruitment design and implementation and who can play an important role in determining who gets recruited into a clinical trial study and who does not. To illustrate, a recent survey examining perceptions of and experience with clinical trials among a sample of 4,006 individuals in the United States revealed notable differences in familiarity with clinical trials among groups based on education and income level.
Specifically, those with less than a high school education were less likely to be familiar with clinical trials and less likely to have been asked to participate in a clinical trial compared to those who were more educated. Additionally, the same study revealed that there was a notable contrast in how people from different SES groups were informed about clinical trials.
When asked about the top two ways through which they found out about clinical trials, all groups, regardless of their education or income level, shared that the most common way they found out about clinical trials was through email. However, the second most common method is where differences began to emerge: those with an annual income above $40,000 shared that the second most common way they find out about clinical trials was through their physician, whereas those who had an annual income of less than $40,000 were more likely to find out about clinical trials via social media.
Similar patterns of referral methods emerged by race—the most common method that individuals, regardless of their racial background, found out about clinical trials was through email. However, for White participants, the second most common way of learning about clinical trials was through their physicians, whereas for patients of color—including Black, Latino, and Asian participants—the second most common way of learning about clinical trials was through social media or referral from family/friends, not from their physicians.
These findings highlight that current recruitment practices may be highly susceptible to subjectivity and warrants further investigation into existing recruitment practices and enrollment strategies among clinical research sites where most clinical trials are being conducted. As part of an effort to map baseline recruitment and enrollment strategies, Tufts Center for the Study of Drug Development launched a working group study comprised of 15 biopharmaceutical and contract research organizations to survey clinical research sites in the United States about their recruitment and enrollment practices and whether their strategies targeted socioeconomically disadvantaged patients. The study was sponsored by Parexel.
The online survey was launched using the Qualtrics survey platform and received 504 responses. Data collection lasted approximately three months. Principal investigators (PIs) were the largest group of site representatives responding to the survey (35.6%), with clinical research coordinators (CRCs) and clinical research nurse coordinators (CRNCs) also making up a large proportion of the dataset (29.7%). The remaining responses were completed by administrative personnel or other site personnel.
Many of the sites responding to the survey were located in the Southern United States (47.3%) and in urban areas (94.4%). Private/for-profit sites, which made up 57.5% of the dataset, were defined as any site identifying as: standalone, dedicated research sites; private or group practices; for-profit clinic, hospital, or healthcare system; and sites that were part of a research site network. Public/non-profit sites (42.5%) included university-affiliated hospital or academic medical centers; and non-profit or government-affiliated clinics, hospitals, or health systems.
The study results revealed several insights. First, although approximately half of the sites shared that they use patient demographic data to inform their recruitment plan and had some type of parameter to ensure that recruitment plans included patients from different socioeconomic backgrounds, most sites did not collect socioeconomic data about their patients.
Whereas between 81% and 98% of sites reported that they collect patients’ age, race, and gender, only 41% of sites collected patient’s education level and less than 10% of sites collected patient’s annual household income level. Socioeconomic status is a known social determinant of health that can influence not only patient attitudes but their health behaviors, as well as their interactions with healthcare providers.6
Not tracking patient socioeconomic information makes it harder not only to diagnose gaps in representation based on income and education but also to tailor recruitment and enrollment strategies that can help close the recruitment gap and make studies more inclusive. This finding suggests that despite the espousal for the need to recruit socioeconomically disadvantaged patients into clinical trials, when it comes to implementation, most sites are operating in the blind by not collecting relevant SES data that could be used to highlight recruitment gaps and bolster recruitment and enrollment strategies.
Another key finding was the lack of collaboration with community-based organizations to recruit hard-to-reach populations. Despite the literature that shows the effectiveness of using community-based partnerships to close the participation gap,7 our findings showed that most sites do not use any form of community-based partnerships in their recruitment efforts.
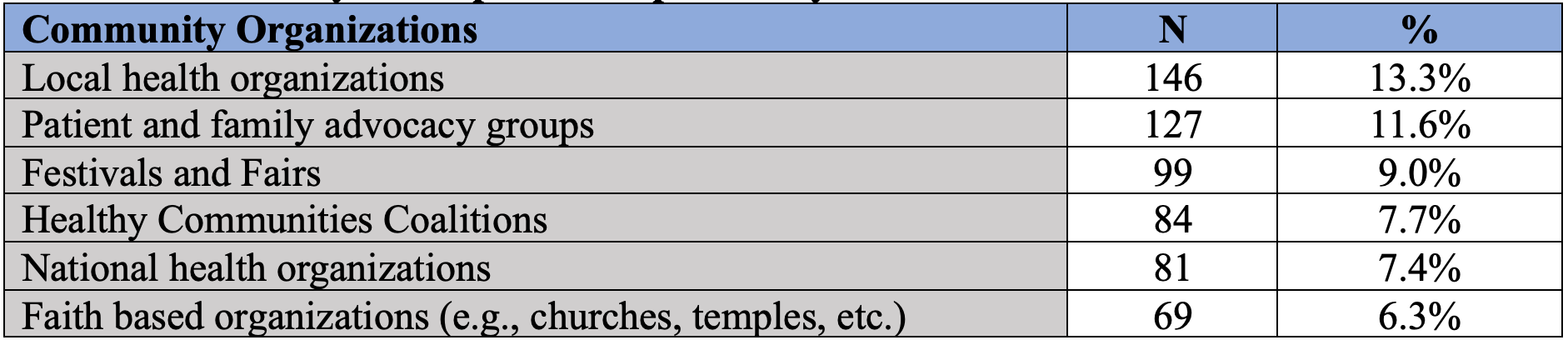
For example, only 13% of respondents shared that they partnered with local health organizations, followed by 12% who partnered with patient and family advocacy groups (Table 1). What this suggests is that community-based organizations are underutilized by most clinical research sites.


Table 1. Community-based partnerships used by clinical research sites
Next, we examined perceived barriers from the site perspective to understand what may be hindering them from collecting and tracking patient SES data. Approximately 53% of the sites felt that they received adequate support from sponsors and/or contract research organizations (CROs) to accommodate the financial needs of patients, while 41.3% felt that they did not receive adequate support (Table 2).
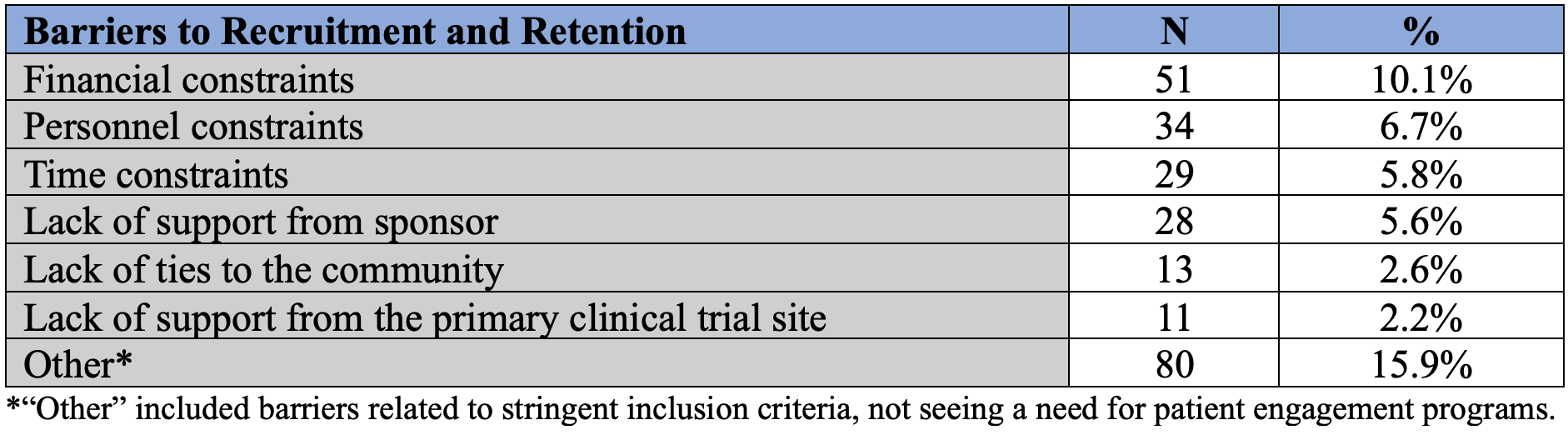
To delve into this further, we looked at perceived barriers related to engaging and supporting patients and found that the top perceived barriers related to financial, personnel, and time constraints, a finding that mirrors previous research showing that resource constraints are often viewed as one of the top barriers for effective recruitment.8 Other barriers that were categorized under “Other” included concerns related to stringent inclusion criteria; inability of patients to pay for studies; lack of knowledge and awareness among patients; as well as lack of urgency among sites that see the need for patient engagement programs.


Table 2. Description of perceived barriers to recruitment and retention of patients by SES status
Mitigating the SES gap in representation
The study highlighted notable gaps among current recruitment practices that shed light on potential reasons for why socioeconomically disadvantaged groups are seldom recruited into clinical trials and how this gap can contribute to health disparities they experience. To tackle this challenge, some organizations have begun to pay more attention to SES as a variable in their recruitment strategies. Below, we share two testimonials from two sponsor organizations and what practices they are incorporating into their overall recruitment strategy to help reduce barriers faced by socioeconomically disadvantaged patients.
Sanofi
At Sanofi, we collaborate internally and externally to build an ecosystem for clinical trial delivery, centered around the patient experience and focused on removing barriers that prevent access to clinical trials. We are taking a deliberate approach to reduce the financial burden of clinical trials for both sites and patients through capacity building, investing in site infrastructure and resourcing, and leveraging technology to deliver clinical trials near or within patient homes. To achieve this, we have enabled a variety of patient-centric tactics including adopting in-home (or office) study visits, providing patient travel and lodging reimbursement, increasing awareness of clinical trials through direct to patient advertising, working with sites to implement flexible study visit hours, and partnering with patient navigators and community health workers.
In addition, we are evaluating the findings from this study, noting that socioeconomic status is an important variable and predictor of patient enrollment, and incorporating these insights into our future strategies around site media awareness and utilizing artificial intelligence (AI) technology to support patient engagement and community partnership.
Genentech
Addressing the lack of socioeconomic status (SES) data in clinical trial recruitment is a crucial step in ensuring that diverse populations are represented and that the outcomes of the trials are applicable to a wide range of individuals. To address these concerns, Genentech has begun implementing initiatives to encourage participation among different SES groups. For instance, we have begun using an optional data collection tool for clinical trial participants to complete at the screening visit. We view this as a proactive step to gather information on their socioeconomic status, which is crucial for tracking and improving the representation of diverse SES backgrounds in trials. These data can guide recruitment efforts and help ensure equitable participation.
Another way to encourage participation among lower income patients is to consistently provide logistical support to encourage participation.Our goal has been to provide transportation assistance, cover the cost of childcare services, and/ or provide reasonable financial compensation for time and travel expenses consistently across studies to help alleviate the financial burden directly associated with participation, making it more feasible for individuals from lower SES backgrounds to participate in clinical trials. This proactive support can remove practical obstacles that may have deterred potential participants.
Finally, we are focusing on community partnerships centered around education—raising awareness about the significance of clinical trials. Our goal is to develop accessible educational materials in various languages and formats to ensure that potential participants understand the trial's purpose, procedures, and potential benefits and risks.
This approach will empower individuals to make informed decisions about their participation and fosters trust in the clinical trial process. This type of community engagement will not only help increase the footprint of clinical trials in community settings but also strengthen ties and ability to recruit underserved communities. Our organization is aiming to implement and scale all of the steps shared consistently across all studies to ensure better representation among socioeconomically disadvantaged patients.
Conclusion
Barriers to participation in clinical trials remain a big problem for historically marginalized groups, which include the less educated and lower income individuals. Our recent study highlights ways in which socioeconomically disadvantaged are being left behind in drug development, while underscoring recruitment strategies that may need to be bolstered.
We have also shared examples of proactive and practical next steps that are being undertaken by sponsor organizations to support clinical research sites in their efforts to provide access to potentially life-saving trials to patients in need (Table 3).


Table 3. Summary of actionable steps that stakeholders can take to improve representation in clinical trials
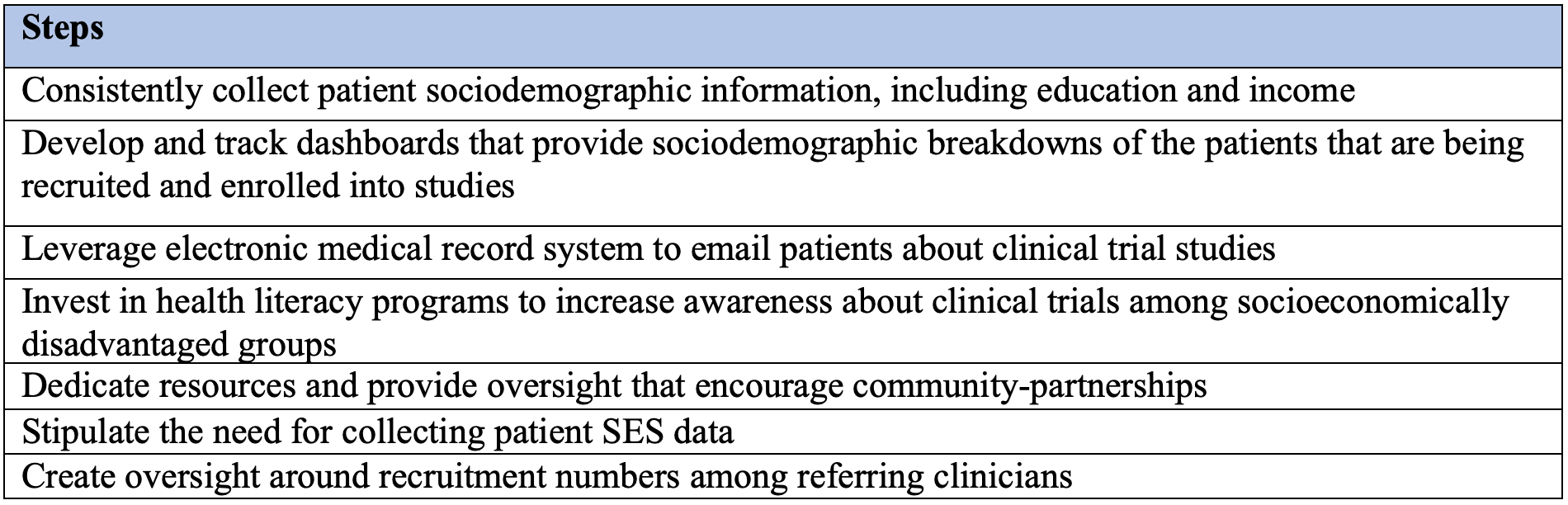
Above all, underpinning the compensation, logistical support, and community partnerships should be the practice of consistently collecting patient sociodemographic data, which can help benchmark baseline metrics that sponsors, CROs, and sites should work together to track to ensure that they are providing opportunities for patients of all SES backgrounds to expand their treatment options and improve their overall health.
Acknowledgment statement. The authors thank Ken Getz at Tufts CSDD for his advising role on the study. We thank Parexel for sponsoring the study. The authors also thank representatives from the following organizations for providing their support as part of the working group: AbbVie; Astellas; AstraZeneca; Bayer; Biogen; CSL Behring; EMD Serono; Gilead; GSK; Otsuka; Pfizer; Parexel; Genentech, a member of the Roche Group; Sanofi; Takeda; and UCB.
References
1. Unger JM, Vaidya R, Hershman DL, Minasian LM, Fleury ME. Systematic Review and Meta-Analysis of the Magnitude of Structural, Clinical, and Physician and Patient Barriers to Cancer Clinical Trial Participation. JNCI: Journal of the National Cancer Institute. 2019;111(3):245-255. doi:10.1093/jnci/djy221
2. Diversity and Inclusion in Clinical Trials. NIMHD. Accessed October 6, 2023. https://nimhd.nih.gov/resources/understanding-health-disparities/diversity-and-inclusion-in-clinical-trials.html
3. Baquet CR, Commiskey P, Daniel Mullins C, Mishra SI. Recruitment and participation in clinical trials: Socio-demographic, rural/urban, and health care access predictors. Cancer Detection and Prevention. 2006;30(1):24-33. doi:10.1016/j.cdp.2005.12.001
4. Niranjan SJ, Martin MY, Fouad MN, et al. Bias and stereotyping among research and clinical professionals: Perspectives on minority recruitment for oncology clinical trials. Cancer. 2020;126(9):1958-1968. doi:10.1002/cncr.32755
5. Kim JY, Florez M, Botto E, Belgrave X, Grace C, Getz KA. The impact of socioeconomic status on individual attitudes and experience with clinical trials: How socioeconomically disadvantaged individuals are being left behind. Published online Under Review.
6. Tufts Center for the Study of Drug Development. Impact Report: Select Socioeconomic Factors Highly Associated with Clinical Trial Attitudes and Interest. Tufts University; 2023.
7. Bodicoat DH, Routen AC, Willis A, et al. Promoting inclusion in clinical trials—a rapid review of the literature and recommendations for action. Trials. 2021;22(1):880. doi:10.1186/s13063-021-05849-7
8. Bull J, Uhlenbrauck G, Mahon E, Furlong P, Roberts J. Barriers to Clinical Trial Recruitment and Possible Solutions: A Stakeholder Survey. Applied Clinical Trials Online. Published September 3, 2015. Accessed October 6, 2023. https://www.appliedclinicaltrialsonline.com/view/barriers-clinical-trial-recruitment-and-possible-solutions-stakeholder-survey












Improving Relationships and Diversifying the Site Selection Process
April 17th 2025In this episode of the Applied Clinical Trials Podcast, Liz Beatty, co-founder and chief strategy officer, Inato, discusses a number of topics around site engagement including community-based sites, the role of technology in improving site/sponsor relationships, how increased operational costs are impacting the industry, and more.

Putting Collective Insights Into Action to Advance Cancer Care: Key Examples From ASCO 2025
June 27th 2025At ASCO 2025, clinical operations leaders gained critical insights into how AI tools, bispecific antibodies, and evolving treatment paradigms are reshaping trial design, endpoint selection, and patient stratification.

Reaching Diverse Patient Populations With Personalized Treatment Methods
January 20th 2025Daejin Abidoye, head of solid tumors, oncology development, AbbVie, discusses a number of topics around diversity in clinical research including industry’s greatest challenges in reaching diverse patient populations, personalized treatment methods, recruitment strategies, and more.



