Diversity by Design: Combining Strategic Protocol Planning with Accurate Real-world Data
Leveraging a “diversity by design” approach can build patient narratives and optimize protocols from the onset.



Sanofi has been partnering with TriNetX, a global health research network that propels clinical research and empowers scientific discoveries through real-world evidence (RWE). Partnering together allows Sanofi to leverage real world data (RWD) as one mechanism, to improve clinical trial diversity. The approach aims to minimize the introduction of unintentional bias in protocol designs that can occur when following a conventional, protocol-first approach, focused only on total patient numbers. This necessitated a paradigm shift from assessing the impact of diversity within the protocol after it is authored and study initiation to examining disease demographics and patient journeys to shape the protocol from the onset.
In this article, we will discuss how RWD can inform trial design, specifically, to optimize for diverse representation and identify the downstream strategies and tactics for early patient engagement and recruitment.
Unbalanced representation in clinical trials and its impact
Clinical trial participation today is not representative. Between 2000 and 2020, only 43% of trials listed on www.clinicaltrials.gov reported any race or ethnicity data.1,2 Factors that have led to this imbalance include limited or no reporting on demographics, lack of access to trial sites, limited patient awareness, barriers pervading culture, structures, and social determinants, and mistrust across different communities.
Why is it important?
Beyond the obvious and paramount ethical concerns, when trials are not representative, the generalizability of the research findings is reduced. People from different races, ethnicities, age groups, and genders can vary in their disease presentation and underlying health, ultimately impacting how they respond to a treatment. Lack of evidence concerning these variable responses has a measurable impact on individual communities, and on society as a whole.2 Failure to address common disorders impacts quality of life including working life.
Finding opportunities to improve representation
It is well documented in literature that improving representation requires a multifactorial approach that includes building trust, selection of clinical trial sites located in traditionally underserved communities, and reducing the burden of trial participation (e.g., costs, transportation, and wages for lost work time).1,3 Additionally, complex inclusion and exclusion criteria in clinical trial protocols may create unintentional ineligibility which must also be factored into these solutions.4,5,6
More representative clinical trials can be achieved through diversity by design at the earliest stages of trial development.
Building the patient experience narrative
To address the current imbalance of representation in clinical trials, a multifactorial approach is needed. At Sanofi, our approach begins by building the patient experience narrative.
At the time a disease or condition is identified for study, a patient experience narrative is developed, which summarizes descriptive data about the people who have that diagnosis.
At minimum, it includes the following:
- Epidemiological and demographic data,
- Comorbidities and risk factors,
- Cytogenetic/molecular factors for stratification,
- Patient segmentation, classification, or staging information,
- Descriptions of social, racial, and ethnic determinants having impact on symptoms, diagnosis, treatment, prognosis, or outcomes,
- Voice of the patient.
The patient experience narrative (example in Figure 1) is then used to inform development and operations teams by clearly and accurately conveying unmet patient needs and surfacing any differences or disparities between sub-populations.


Figure 1. Example of a Patient Narrative
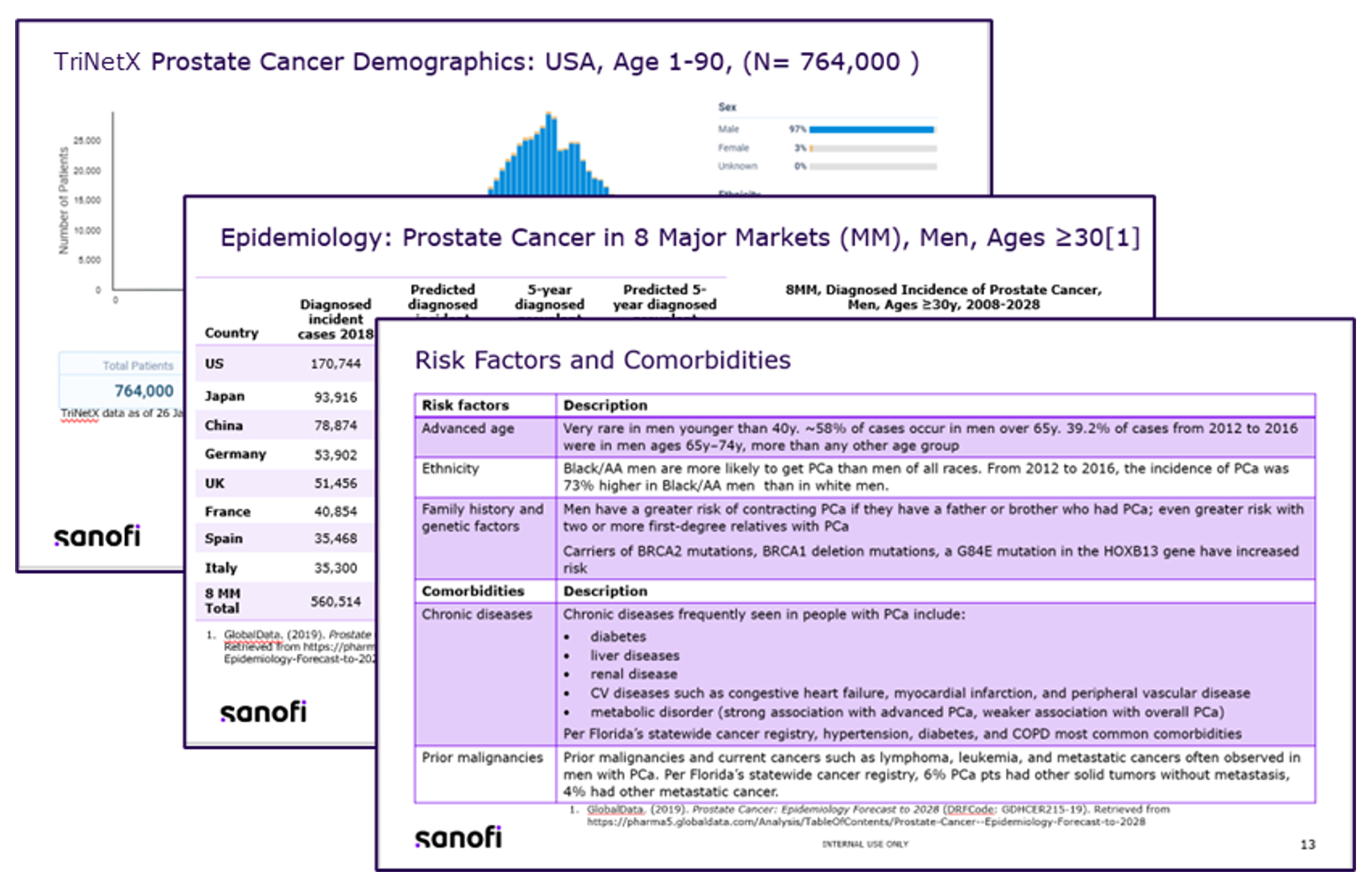
Early insights build a strong foundation for representative trials
Once we have the patient experience narrative in place, we continue to use a variety of data sources (clinicaltrials.gov, TriNetX data, primary literature, and US census data) to assess how planned inclusion and exclusion criteria may differentially impact sub-populations and obtain a real-time map of trial sites with appropriate demographic diversity.
Utilizing robust data sets and analytics platforms, such as TriNetX, is critical in enabling development teams to assess patient population, extrapolate for comparison to primary literature and other sources, including US census data, and confidently establish diversity goals (example in Figure 2).


Figure 2. Diversity Goal Setting Executive Summary: Atopic Dermatitis
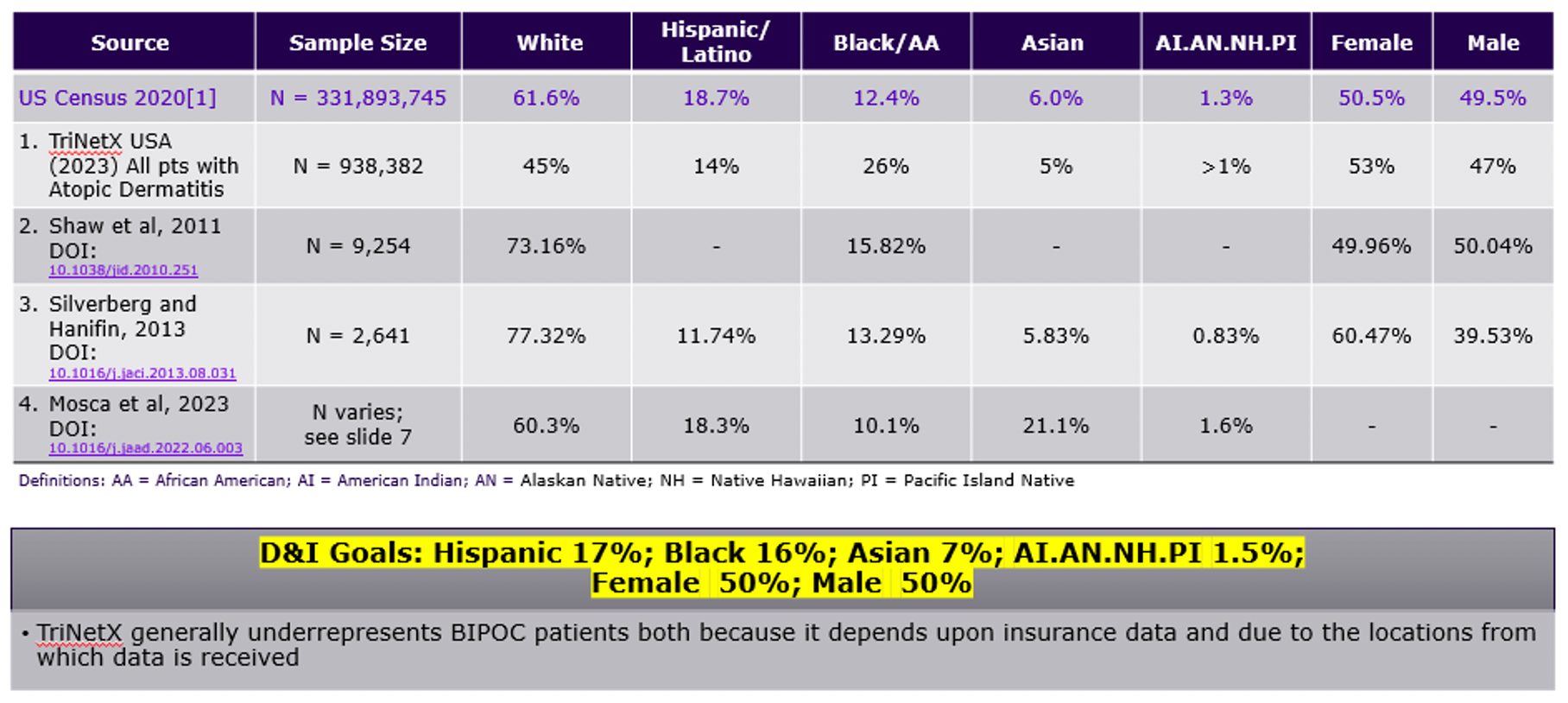
Once goals are defined, analytical platforms allow us to precisely refine protocols to match our patient experience narrative. Demographics inclusive of (age, gender, race and ethnicity), geographic, health outcome, and social determinants of health data are assessed while iterating on and optimizing inclusion and exclusion criteria.
Example: Modifying exclusion criteria to reduce barriers
If we are considering excluding patients from a clinical trial because they have diabetes, we use TriNetX data to understand how this might impact groups that may have a greater prevalence of diabetes. If the criterion creates a barrier for participation for one or more groups, we can use a variety of strategies to correct this imbalance and/or adjust the planned trial locations.
Augmenting the trial by site geography or by modifying inclusion and exclusion criteria with greater nuance, inadvertently avoids penalizing people from underrepresented groups. Steps are taken to make modifications that won’t impact the efficacy or safety of the investigational drug. For example, we might factor in the extent to which their diabetes is under control.
Modeling cohorts and site/country mix
Assessment of comorbidities is another useful method for viewing data and optimizing protocols for representation within TriNetX. We build cohorts made up of individual races, holding all other factors constant, and compare similar comorbidities between cohorts.
Matching trial sites to the intended study population is essential for study recruitment. Again, analytics platforms provide another source of data-driven insights as to the locations where individuals living with the disease under study are being treated. The trialists at these centers are also able to evaluate the clinical trial protocol and more easily determine if it is a health care option for individuals in their practices or community.
Using these steps, we are already seeing success. This methodology has helped us establish goals for all of our recruiting trials and provides additional insights related to the patient healthcare journey as part of D&I planning.
It should be noted that success also requires sponsors to establish strong collaborations with sites imbuing shared vision and trust. Building capabilities with sites from traditionally underrepresented communities may require additional resources and infrastructure investments from both the sponsor and investigational institution.
On the horizon
As a result of building diversity objectives into clinical trial designs from conceptual stages, study teams can further reinforce inclusion goals and planning by proactively engaging site and community stakeholders. These plans include, but are not limited to support that aims to cultivate trust within local communities and mobilize the necessary support mechanisms to make study participation available to those interested.
Additionally, innovative data providers should continue to help fill in gaps that exist across traditional health data measures and consider aggregating novel data sources (e.g., social vulnerability index, etc.) for greater completeness and accuracy efforts to advance D&I.
Conclusion
“Diversity by Design" marks a pivotal shift in clinical trial planning, in leveraging real-world data to build patient narratives and strategically optimizing protocols and fostering diversity from the onset. Intelligently leveraging data allows clinical development teams to proactively combat unintentional biases.
This approach prioritizes early identification of potential barriers and opportunities for enabling diverse representation, ensuring that clinical trials reflect the real-world distribution of disease states across demographic populations. The integration of patient narratives and robust data analysis enhances trial inclusivity and bolsters the reliability and applicability of research findings across varied populations.
Victoria A. DiBiaso, Sanofi 1 Avenue Pierre Brossolette, Chilly Mazarin, France
Beth Brooks and Monique R. Adams, Sanofi, 55 Corporate Dr, Bridgewater, NJ, USA
Conflict of Interest
Victoria A DiBiaso, Mary Elizabeth Brooks, and Monique Adams are employees and may hold stock and/or stock options in Sanofi.
Author contributions
All authors were involved in the design of the study, data analysis, and interpretation. Victoria DiBiaso developed the initial draft of the manuscript; all other authors supported the critical review and development of the final drafts. All the authors critically reviewed and approved the final manuscript draft for publication.
References
- Turner, B. E., Steinberg, J. R., Weeks, B. T., Rodriguez, F., & Cullen, M. R. (2022). Race/ethnicity reporting and representation in US clinical trials: a cohort study. Lancet Reg Health Am, 11. doi:10.1016/j.lana.2022.100252
- Academies of Sciences, E., and Medicine,. (2022). Improving Representation in Clinical Trials and Research: Building Research Equity for Women and Underrepresented Groups. Washington, DC: The National Academies Press.
- Chen, M. S., Jr., Lara, P. N., Dang, J. H., Paterniti, D. A., & Kelly, K. (2014). Twenty years post-NIH Revitalization Act: enhancing minority participation in clinical trials (EMPaCT): laying the groundwork for improving minority clinical trial accrual: renewing the case for enhancing minority participation in cancer clinical trials. Cancer, 120 Suppl 7(0 7), 1091-1096. doi:10.1002/cncr.28575
- DeCormier Plosky, W., Ne'eman, A., Silverman, B. C., Strauss, D. H., Francis, L. P., Stein, M. A., & Bierer, B. E. (2022). Excluding People With Disabilities From Clinical Research: Eligibility Criteria Lack Clarity And Justification. Health Aff (Millwood), 41(10), 1423-1432. doi:10.1377/hlthaff.2022.00520
- Peters, U., Turner, B., Alvarez, D., Murray, M., Sharma, A., Mohan, S., & Patel, S. (2023). Considerations for Embedding Inclusive Research Principles in the Design and Execution of Clinical Trials. Ther Innov Regul Sci, 57(2), 186-195. doi:10.1007/s43441-022-00464-3
- Roy, E., Chino, F., King, B., Madu, C., Mattes, M., Morrell, R., . . . Ludwig, M. (2023). Increasing Diversity of Patients in Radiation Oncology Clinical Trials. Int J Radiat Oncol Biol Phys, 116(1), 103-114. doi:10.1016/j.ijrobp.2022.11.044











Putting Collective Insights Into Action to Advance Cancer Care: Key Examples From ASCO 2025
June 27th 2025At ASCO 2025, clinical operations leaders gained critical insights into how AI tools, bispecific antibodies, and evolving treatment paradigms are reshaping trial design, endpoint selection, and patient stratification.

Unifying Industry to Better Understand GCP Guidance
May 7th 2025In this episode of the Applied Clinical Trials Podcast, David Nickerson, head of clinical quality management at EMD Serono; and Arlene Lee, director of product management, data quality & risk management solutions at Medidata, discuss the newest ICH E6(R3) GCP guidelines as well as how TransCelerate and ACRO have partnered to help stakeholders better acclimate to these guidelines.


Improving Relationships and Diversifying the Site Selection Process
April 17th 2025In this episode of the Applied Clinical Trials Podcast, Liz Beatty, co-founder and chief strategy officer, Inato, discusses a number of topics around site engagement including community-based sites, the role of technology in improving site/sponsor relationships, how increased operational costs are impacting the industry, and more.

Beyond the Molecule: How Human-Centered Design Unlocks AI's Promise in Pharma
June 23rd 2025How human-centered AI that is focused on customer, user, and employee experience can drive real transformation in clinical trials and beyond by aligning intelligent technologies with the people who use them.

